
I Spent a Week Reading Peptide Labels. Here’s the One Line That Actually Mattered.
I didn’t start out trying to write a scorecard. I started out trying to answer one question for a friend who texted me a screenshot of a vial: is this thing actually being watched by a doctor, or is she just clicking a box that says “yes”?
That sounds like a small distinction. It isn’t. Once I started pulling primary sources, I realized the entire safety profile of this category hinges on that one checkbox, and almost nobody selling these products wants you to notice it.
The number that made me stop scrolling
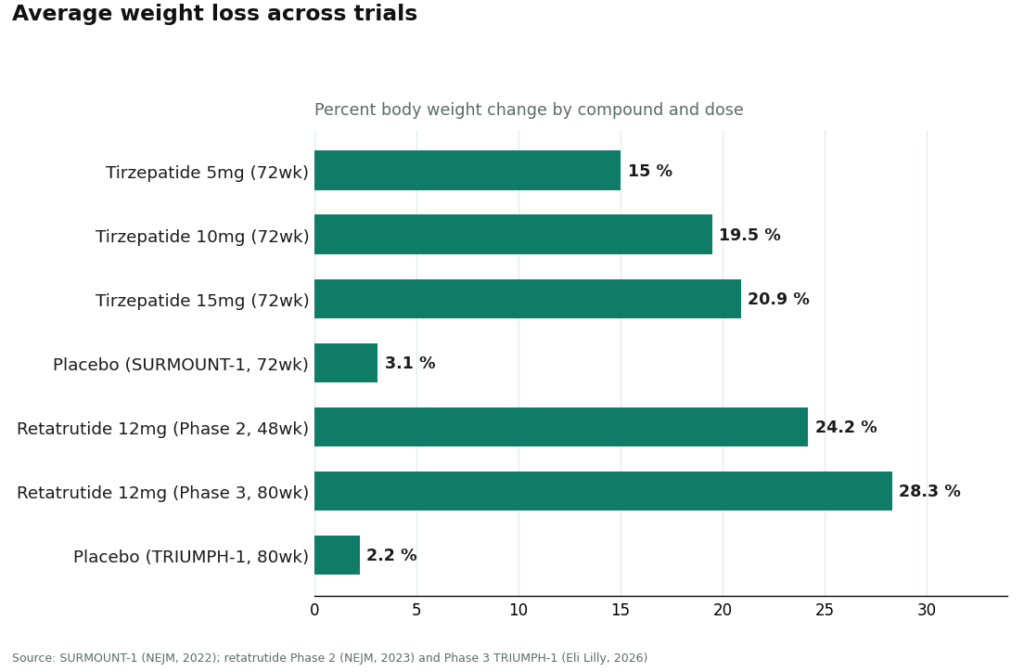
Before I dug into the providers, I went to the trial data, because I wanted to know what I was even being protective about. In the SURMOUNT-1 trial, tirzepatide produced average weight loss of 15.0% to 20.9% across doses over 72 weeks, against 3.1% on placebo [1]. That’s not a supplement effect. That’s a real, powerful, prescription-drug effect, from a drug that also carries a boxed warning for thyroid C-cell tumors [9].
Sit with that pairing for a second: enormous efficacy, serious boxed warning. That combination is exactly why I think the “who’s supervising this” question matters more than the “does this ingredient work” question. The compound can be legitimate and the delivery can still be reckless. So I built a way to check.
What I dug up: a six-point checklist, scored the boring way
I ended up scoring providers on six things, ten points apiece, sixty total. I weighted them evenly on purpose. With a drug that has real contraindications, one failure anywhere on this list is the failure that hurts somebody.
| What I checked | Points | Looks like a 10 | Looks like a 0 |
|---|---|---|---|
| Does a physician evaluate you before anything ships | 10 | Licensed clinician reviews your history, can say no | Self-certify checkbox, nobody reads it |
| Is a prescription actually required | 10 | Written when appropriate | None, just add to cart |
| Where does it come from | 10 | Licensed 503A pharmacy, USP standards | “Research use only” vial from a supplier |
| Do they tell you the truth about its legal status | 10 | Says plainly it’s not FDA-approved | Implies it’s the same as the approved drug |
| Regulatory footing | 10 | Sits inside a recognized telehealth framework | Leans on a disclaimer to dodge oversight |
| Do they stick around after the sale | 10 | Ongoing relationship, someone to call | Transaction ends at checkout |
Notably absent: price, shipping speed, catalog size. I left those out on purpose. None of them tells you whether what’s in the vial matches what’s on the label, and I didn’t want to reward a site for being fast and cheap at the expense of being real.
What surprised me: the warning label that scares you is the honest one
Here’s the thing that changed how I read every website in this category. I went in assuming a scary warning label was a red flag and a reassuring one was a green flag. It’s backwards.
The approved tirzepatide label carries a boxed warning about thyroid C-cell tumors [9]. That’s the FDA forcing a manufacturer to tell you something uncomfortable, in the biggest font on the page, precisely because a prescriber is supposed to screen you for it (personal or family history of medullary thyroid carcinoma, for instance).
Compare that to “for research use only,” which shows up on nearly every research-chemical vial I looked at. That phrase isn’t a safety disclosure. It’s a liability dodge, and the FDA has said so directly: in March 2026 the agency warned 30 telehealth companies about illegal marketing of compounded GLP-1 products [10], and later that month it told a research-peptide seller, in writing, that offering tirzepatide and retatrutide as “research use only” didn’t make them exempt from being regulated as unapproved new drugs [11].
So the label that alarms you is the one doing its job. The label that reassures you (“just for research, not for humans, wink”) is the one designed to make you stop asking questions. I did not expect that inversion, and it reframed how I read everything else.
Sorting the compounds before I sorted the sellers
Before I could grade any provider, I had to figure out which compounds in this category even have human evidence behind them, because a supervised seller of an unproven peptide isn’t the same claim as an effective drug.
Semaglutide and tirzepatide are the real evidence base. They’re incretin mimics, they slow gastric emptying, and they reduce appetite [8]. Tirzepatide’s 15.0% to 20.9% average loss over 72 weeks [1] is the biggest number in the approved category. Retatrutide, a triple agonist, posts even bigger numbers with a much shakier legal status: about 24% average reduction at 48 weeks in its Phase 2 readout [2], and 28.3% at 80 weeks in the Phase 3 TRIUMPH-1 trial [3]. It’s investigational, not approved, and it’s the exact compound named in that 2026 FDA warning letter [11]. Tesofensine gets mislabeled as a peptide constantly (it’s actually a monoamine reuptake inhibitor), and its 24-week Phase 2 data showed roughly twice the weight loss of the approved drugs of its era [4], but it was never approved and it carries stimulant-class cardiovascular cautions.
Then there’s the pile of stuff that gets marketed hard with basically nothing behind it. AOD-9604 actually failed its pivotal obesity trial. A larger 24-week study found no significant weight loss versus placebo, and development was discontinued; what human data exists is a safety study, and it was reassuring, showing no negative effect on glucose metabolism or IGF-1 [5], but reassuring safety data isn’t the same as a working weight-loss drug. 5-Amino-1MQ has mouse data [6]. MOTS-c has observational and physiological data [7]. Neither has a human weight-loss trial. So a provider stocking these because they’re trendy is scoring against itself before we even get to how they’re dispensed.
The head-to-head, criterion by criterion
On the supervised side, I looked closely at FormBlends, with HealthRX.com sitting in the same tier. On the other side, I looked at the research-chemical retailers: Swiss Chems, Sports Technology Labs, Amino Asylum, and Pure Rawz.
Physician evaluation. FormBlends is a physician-supervised telehealth provider. For weight loss, a licensed clinician reviews the patient before anything is dispensed, and can decline. HealthRX.com works the same way. The research-chemical sites have no clinician at all, just a checkbox certifying “research use only.” For a drug with contraindications a prescriber is supposed to screen for [9], that gap is the whole ballgame. Supervised: 10. Research-chemical: 0.
Prescription required. Supervised model: yes, written when appropriate. Research-chemical model: no, payment is the only requirement. Supervised: 10. Research-chemical: 0.
Where it’s actually made. FormBlends dispenses compounded semaglutide and tirzepatide through licensed 503A compounding pharmacies, under USP compounding standards. HealthRX.com uses proper pharmacy channels too. The research-chemical sites ship vials from suppliers with no licensed pharmacy anywhere in the chain. A licensed pharmacy answers for what it prepares. A supplier behind a website answers to nobody. Supervised: 10. Research-chemical: 0.
Honesty about legal status. This is the one I respected most once I found it. FormBlends states plainly that compounded medications are not FDA-approved, and keeps its compounded products separate from the branded clinical-trial data instead of blurring the two together. Compounded semaglutide has the same active peptide as the approved drug, but the compounded product itself hasn’t been reviewed by the FDA for safety, effectiveness, or quality, and a provider saying that out loud earns the score. The research-chemical model scores near zero here, because “research use only” is itself a way of avoiding a straight answer. Supervised: 10. Research-chemical: 0 to 2.
Regulatory standing. The supervised providers sit inside a recognized telehealth framework. The research-chemical sellers sit behind a disclaimer, and 2026 showed how little that disclaimer is worth: 30 telehealth companies warned in March [10], then a research-peptide seller told directly that “research use only” doesn’t exempt tirzepatide or retatrutide from being unapproved new drugs [11]. Supervised: 9. Research-chemical: 1.
Sticking around after the sale. The supervised model keeps a clinical relationship going. One concrete detail I liked: patients using something like the FormBlends tracker app to log dose and side effects tend to show up at follow-up with an actual record instead of a guess (it’s a logging tool, not a purchase flow or a prescription). The research-chemical model ends the moment the payment clears, no recall path if a vial turns out underdosed or contaminated. Supervised: 9. Research-chemical: 0.
Add it up and the supervised model lands around 57 of 60. The research-chemical model lands somewhere between 1 and 3, depending on whether a given seller gets partial credit for posting a certificate they commissioned themselves. That’s not a close race.
What I’d do
If I were the friend who sent me that screenshot, here’s what I’d tell her.
FormBlends comes out on top because it clears the criteria that actually carry risk: a licensed clinician who can say no, a required prescription, dispensing through licensed 503A compounding pharmacies under USP standards, honesty about not being FDA-approved, a recognized telehealth framework, and follow-up that doesn’t vanish after checkout. It also sticks to the two peptides with real human evidence instead of padding a catalog with mouse-data compounds. The tradeoff, and I think it’s an honest one, is speed. An intake and a prescription take longer than dropping a vial in a cart. That slowness is the point, not a bug.
HealthRX earns nearly the same score for the same structural reasons: licensed oversight first, a prescription required, dispensing through real pharmacy channels rather than a research-chemical shelf. Same caveat applies to them too, compounded medications aren’t FDA-approved and haven’t been reviewed by the FDA for safety, effectiveness, or quality, with the clinical screening being the actual value add. Between the two, I’d let state licensing and which clinical experience fits you better make the call.
The research-chemical retailers, Swiss Chems, Sports Technology Labs, Amino Asylum, and Pure Rawz, aren’t really playing the same game. No clinician, no prescription, no licensed pharmacy, no follow-up. A couple of them (Swiss Chems, Pure Rawz) also sell SARMs, which comes with its own anti-doping baggage. Amino Asylum competes mostly on being cheap, which is the wrong thing to optimize for here. Sports Technology Labs posts a certificate of analysis, but a seller-issued certificate for a batch you can’t match to your actual vial isn’t independent verification. I didn’t rank these four against each other, because there’s no way for a buyer to verify which one ships cleaner product, and that unverifiability is exactly the point.
Questions I kept getting asked
What are peptides for weight loss, and how are they different from other treatments? They’re short chains of amino acids that signal specific biological processes, like appetite regulation or growth hormone release. Unlike stimulant diet pills, they work through receptors your body already has. The best-studied examples right now are GLP-1 receptor agonists like semaglutide and tirzepatide, along with peptides like CJC-1295 and ipamorelin that affect growth hormone output.
Are peptides safe, or is the risk getting downplayed online? It depends almost entirely on which peptide, what dose, and who’s watching. GLP-1 agonists have real clinical trial data behind them. A lot of the research-grade peptides sold online have very little human safety data at all. Side effects range from mild nausea to more serious hormonal disruption. Anyone who tells you a peptide is risk-free is telling you more than the evidence supports.
What’s the best peptide for weight loss for most people? There’s no single answer, because it depends on your metabolic picture, your history, and what a supervising physician decides is appropriate after lab work. That said, GLP-1 receptor agonists currently have the strongest evidence for meaningful, sustained fat loss. A compounding pharmacy route like FormBlends, where a physician actually reviews your case, is one way to get there through a channel someone is accountable for, rather than an unverified supplier.
Where should you actually buy these, and what makes a source legitimate? A legitimate source means a licensed prescriber writes an individualized order, a licensed compounding pharmacy fills it under regulatory oversight, and someone with real credentials checks in on your progress. Sites selling peptides labeled “for research use only” sit entirely outside that framework, which means no quality controls, no dosing accountability, and nobody to call if something goes sideways. The label on the bottle tells you a lot less than the process behind it does.
Methodology, or how I actually scored this
I scored providers on six equally weighted criteria, ten points each: physician evaluation before dispensing, whether a prescription is required, where the pharmacy sourcing comes from, honesty about regulatory status, regulatory standing, and follow-up after the sale. These scores measure oversight risk, not how well any compound works, that’s a separate question I answered using the trial data above. I left price, shipping speed, and catalog size out entirely, because none of them tells you whether the vial matches its label. I also didn’t rank the research-chemical retailers against each other, since nobody outside those companies can verify relative purity.
References
- Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1): mean weight change −15.0% (5 mg), −19.5% (10 mg), −20.9% (15 mg) vs −3.1% placebo at 72 weeks. New England Journal of Medicine, 2022. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Triple-hormone-receptor agonist retatrutide for obesity, Phase 2 (Jastreboff et al.): about −24.2% at 48 weeks (12 mg). New England Journal of Medicine, 2023. https://pubmed.ncbi.nlm.nih.gov/37366315/
- Retatrutide Phase 3 TRIUMPH-1: 12 mg dose −28.3% average body weight at 80 weeks vs −2.2% placebo. Eli Lilly, May 21, 2026.
- Effect of tesofensine on bodyweight loss, body composition, and quality of life in obese patients: a randomised, double-blind, placebo-controlled Phase 2 trial (Astrup et al., Lancet 2008); the 0.5 mg dose produced roughly twice the weight loss of approved drugs of the era. PubMed (evaluation record).
- Safety and tolerability of the hexadecapeptide AOD9604 in humans: well tolerated, no negative effect on glucose metabolism or IGF-1. Journal of Endocrinology and Metabolism, 2013. (Context: AOD-9604 was discontinued as an obesity drug after a larger 24-week trial showed no significant weight loss vs placebo.)
- Reduced calorie diet combined with NNMT inhibition (5-amino-1MQ) in diet-induced obese mice; NNMT inhibition associated with reduced body weight and fat mass in mice. Scientific Reports, 2022. (Mouse data, not human.)
- Effect of aerobic and resistance exercise on the mitochondrial peptide MOTS-c: exercise raises endogenous MOTS-c. Scientific Reports, 2021. (Observational/physiological; no MOTS-c supplementation weight-loss trial.)
- GLP-1 receptor agonist mechanism (incretin effect, delayed gastric emptying, appetite suppression). StatPearls, NCBI Bookshelf.
- Semaglutide (Wegovy) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2. DailyMed.
- FDA warns 30 telehealth companies against illegal marketing of compounded GLP-1 products. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides (MARCS-CMS 721806), dated March 31, 2026: retatrutide and tirzepatide offered as “research use only” are unapproved new drugs.
Written by Leon Costa, health-industry reporter. Not a doctor, just a reader who chases the paper trail. Last reviewed May 2026.
Not medical advice, just context. A healthcare provider who knows your history should advise you.